
Virginia Mpox Updates

As of August 19, 2025, 22 mpox cases have been reported to VDH this year. To compare, Virginia had 27 cases in 2024. A concerning increase occurred this July with 13 of the 22 cases being reported. Of 2025 cases, 12 were in the Northern region, five in Central, four in Eastern, and one in Southwest. Among this year’s cases with available information, six of 19 (32%) were in people who recently traveled. This suggests that most infections were locally acquired. Five of 21 (24%) cases were in people with HIV. Thirteen of 19 (68%) were in people who were not vaccinated. As in recent years, most of this year’s cases occurred in adult males.
To date, all mpox cases in Virginia have been caused by Clade II monkeypox virus. This is the strain responsible for the global outbreak that began in 2022. Large Clade I and Clade II outbreaks are occurring, including in Central and Eastern African and in West Africa.
While our local health departments received this update and the below recommendations, we ask our valued community partners to continue to:
-
- Educate the public about mpox prevention and vaccination
- Include mpox in appropriate outreach and education services
- Refer eligible clients to their local health department for vaccination and relevant services
- Download, use, and share VDH mpox digital and print resources
Contact Diana Prat, Deputy Director, Division of Disease Prevention, at diana.prat@vdh.virginia.gov, or 804-864-7961, with any questions about DDP mpox efforts or for additional assistance.
DDP Data Dashboards
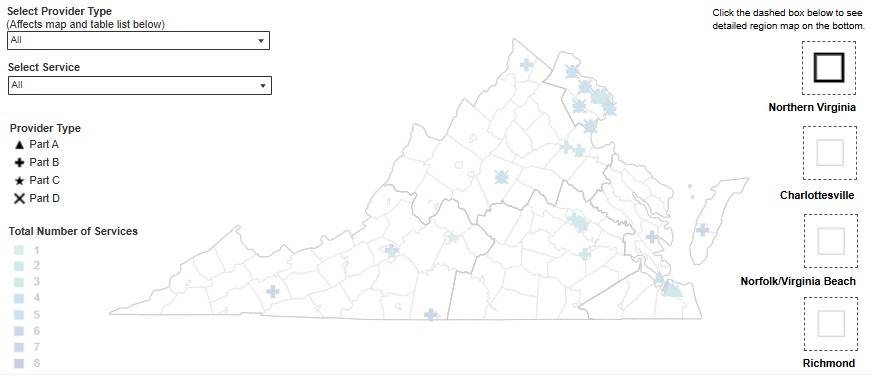 In collaboration with the Division of Informatics and Information Systems (DIIS), DDP has released a new interactive dashboard for Ryan White services. The dashboard is a map of service providers throughout the Commonwealth. It allows users to filter providers by region or service type (part A, B, C, or D). Pop out maps are provided on the map to provide detailed views of areas with higher provider density. You can find the interactive map on the Ryan White Resources page. The webpage includes a description of the different Ryan White parts beneath the map. Please note that this dashboard does not take the place of a service directory and does not contain detailed contact information for agencies. If you see corrections or changes needed to the dashboard, please contact Rivkah Meder at rebecca.meder@vdh.virginia.gov. Updates to the Resource Connections database can be submitted to Brandon Cunningham at brandon.cunningham@vdh.virginia.gov.
In collaboration with the Division of Informatics and Information Systems (DIIS), DDP has released a new interactive dashboard for Ryan White services. The dashboard is a map of service providers throughout the Commonwealth. It allows users to filter providers by region or service type (part A, B, C, or D). Pop out maps are provided on the map to provide detailed views of areas with higher provider density. You can find the interactive map on the Ryan White Resources page. The webpage includes a description of the different Ryan White parts beneath the map. Please note that this dashboard does not take the place of a service directory and does not contain detailed contact information for agencies. If you see corrections or changes needed to the dashboard, please contact Rivkah Meder at rebecca.meder@vdh.virginia.gov. Updates to the Resource Connections database can be submitted to Brandon Cunningham at brandon.cunningham@vdh.virginia.gov.
Additionally, DDP has relaunched the mpox data dashboard. This dashboard is separate from the Monthly Surveillance Report. This will allow for a closer look at mpox data and will get updated weekly, not monthly.
![]()